Learning About Hospice Care
Hospice is a specialized type of care that focuses on supporting individuals who are nearing the end of their life. It provides comfort, pain management, and emotional support to both the patient and their loved ones. Our company understands the importance of dignity, empathy, and compassion in delivering the utmost respect during this sensitive time.
Allegiance Hospice prioritizes in treating each individual with the utmost care and respect, ensuring that their wishes and needs are honored. Our team of compassionate professionals are dedicated to providing personalized care and support, creating a peaceful and comfortable environment for our patients. We strive to foster open communication, listening attentively to the concerns and desires of both the patient and their family. Our goal is to ensure that every person in our care feels valued, heard, and supported throughout their hospice journey. Click on this Video to learn more on Hospice.
Common Hospice Dx & Qualifiers
Patients are eligible for hospice care when their physician determines the patient has a life expectancy of six months or less. The determinants within this guide are to be used as guidelines and should not take the place of a physician’s clinical judgment. When curative treatment is no longer available, hospice can be a beneficial care option for patients and a tremendous source of emotional and physical support for their families. Hospice care includes a full range of services, including medical, pharmaceutical, social and spiritual support. In the absence of one or more of these findings, rapid decline or comorbidities may also support eligibility for hospice care.
Alzheimer's Disease
The patient has both 1 and 2:
- Stage VII or beyond according to the Functional Assessment Staging Scale* with all the following:
- Improperly putting on clothes without assistance or cueing (e.g., may put street clothes on overnight clothes, or put shoes on the wrong feet, or have difficulty buttoning clothing) occasionally or more frequently over the past weeks*
- Unable to bathe properly (e.g., difficulty adjusting the bath water temperature) occasionally or more frequently over the past weeks.*
- Inability to handle mechanisms of toileting (e.g., forgets to flush the toilet, does not wipe properly or properly dispose of toilet tissue) occasionally or more frequently over the past weeks.*
- Urinary incontinence (occasionally or more frequently over the past weeks).*
- Fecal incontinence (occasionally or more frequently over the past weeks).*
- Supporting Evidence for Hospice Eligibility:
- Aspiration pneumonia
- Pyelonephritis or other upper urinary tract infection
- Septicemia
- Decubitus ulcers, Multiple and/or Stage 3-4
- Fever, recurrent after antibiotics
- Inability to maintain sufficient fluid and caloric intake demonstrated by either of the following:
- 10% weight loss during the previous six (6) months, or
- Serum albumin <2.5 gm/dl
*See Functional Assessment Scaling Scale
Functional Assessment Staging (FAST)
Check highest consecutive level of disability:
- No difficulty either subjectively or objectively.
- Complains of forgetting of location of objects. Subjective work difficulties.
- Decreased job functioning evident to co-workers. Difficulty in traveling to new locations. Decreased organizational capacity.*
- Decreased ability to perform complex tasks (e.g., planning dinner for guests, handling personal finances [such as forgetting to pay bills], difficulty marketing, etc.).*
- Requires assistance in choosing proper clothing to wear for the day, season, or occasion (e.g., patient may wear the same clothing repeatedly unless supervised).*
- Occasionally or more frequently over the past weeks for the following*
- Improperly putting on clothes without assistance or cueing.
- Unable to bathe properly (not able to choose proper water temp)
- Inability to handle mechanics of toileting (e.g. forgot to flush the toilet, does not wipe properly or properly dispose of toilet tissue)
- Urinary incontinence
- Fecal incontinence
- Ability to speak limited to approximately ≤ intelligible different words in the course of an average day or in the course of an intensive interview.
- Speech ability is limited to the use of a single intelligible word in an average day or in the course of an intensive interview.
- Ambulatory ability is lost (cannot walk without personal assistance).
- Cannot sit up without assistance (e.g., the individual will fall over if there are not lateral rests [arms] on the chair).
- Loss of ability to smile.
- Loss of ability to hold up head independently.
*Scored primarily on the basis of information obtained from a knowledgeable informant. Psychopharmacology Bulletin, 1988; 24:653-659
Amyotrophic Lateral Sclerosis (ALS)
The patient meets at least one of the following:
- Severely impaired breathing capacity with any of the following findings:
- Dyspnea at rest
- Requirement for supplemental oxygen at rest
- The patient declines artificial ventilation or use of accessory respiratory musculature
- Rapid disease progression with either a or b below. Rapid disease progression as evidenced by any of the following in the preceding twelve (12) months:
- Progression from independent ambulation to wheelchair or bed-bound status
- Progression from normal to barely intelligible or unintelligible speech
- Progression from normal to pureed diet
- Progression from independence in most or all Activities of Daily Living (ADLs) to needing major assistance by caretaker in all ADLs
- Severe nutritional impairment demonstrated by any of the following in the preceding twelve (12) months:
- Oral Intake of nutrients and fluids insufficient to sustain life
- Continuing weight loss
- Dehydration or hypovolemia
- Absence of artificial feeding methods
- Life-threatening complications demonstrated by one or more of the following in the preceding twelve (12) months:
- Recurrent aspiration pneumonia (with or without tube feeding) Upper Urinary Tract Infection (Pyelonephritis)
- Sepsis
- Recurrent fever after antibiotic therapy
- Stage 3 or Stage 4 decubitus ulcer(s)
Cancer
The patient has 1: (a or b) and 2: (c or d)
- Stage VII or beyond according to the Functional Assessment Staging Scale* with all the following:
- a. Disease with metastases at presentation or
- b. Progression from an earlier stage of disease to metastatic disease with either
- c. A continued decline despite therapy; or
- d. Patient declines further disease directed therapy
CVA / Stroke or Coma
The patient has both 1 and 2:
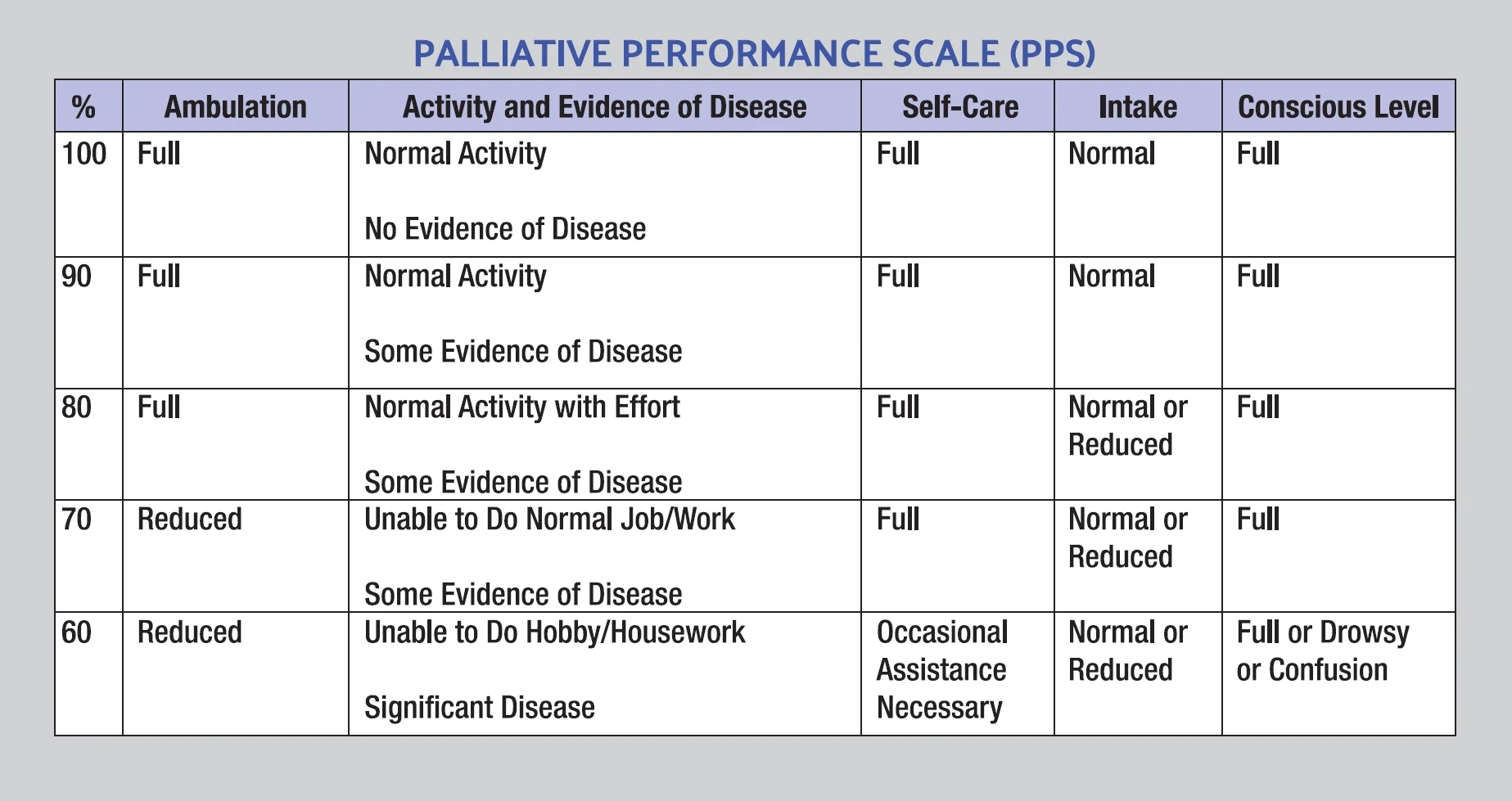
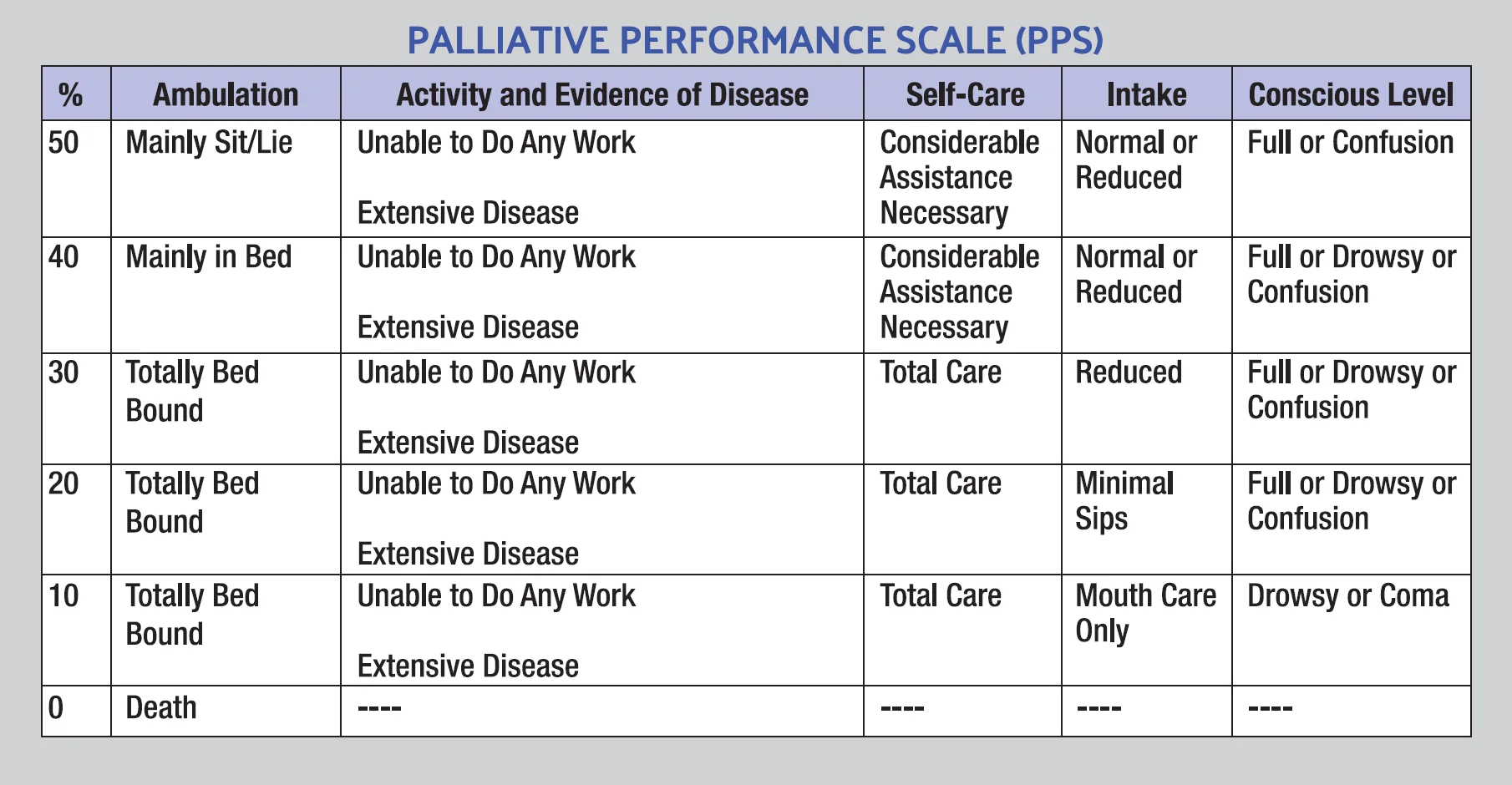
- Poor functional status with Palliative Performance Scale* of 50% or less (Unable to care for self)
- Poor nutritional status with inability to maintain sufficient fluid and caloric intake with either:
- 10% weight loss over the previous six (6) months
- >7.5% weight loss over the previous three (3) months
- Serum albumin <2.5 gm/dl
- Current history of pulmonary aspiration without effective response to speech language pathology interventions to improve dysphagia and decrease aspiration events.
- Dysphagia severe enough to prevent patient from continued fluids/food necessary to sustain life.
Supporting evidence for hospice eligibility:
- Abnormal brain stem response
- Absent verbal responses
- Absent withdrawal response to pain
- Serum creatinine >1.5 gm/dl
Heart Disease / CHF
The patient has 1 or 2, and 3:
- Poor response to (or patient’s choice is not to pursue) optimal treatment with diuretics, vasodilators, and/or angiotensin converting enzyme (ACE) inhibitors, or
- The patient has angina pectoris at rest, resistant to standard nitrate therapy and is not a candidate for invasive procedures and/or has declined revascularization procedures, and
- New York Heart Association (NYHA)* Class III symptoms with both of the following:
- The presence of significant symptoms of recurrent Congestive Heart Failure (CHF) and/or angina at rest
- Inability to carry out even minimal physical activity without symptoms of heart failure (dyspnea and/or angina)
Supporting evidence for hospice eligibility:
- Echo demonstrating an ejection fraction of 20% or less
- Treatment resistant symptomatic dysrhythmias
- History of unexplained or cardiac related syncope
- CVA secondary to cardiac embolism
- History of cardiac arrest or resuscitation
Liver Disease
The patient has both 1 or 2:
1. Synthetic failure as demonstrated by (a), or (b) and (c):
- a. Prothrombin time (PTT) prolonged more than five (5) seconds over control, or
- b. International Normalized Ratio (INR) >1.5, and
- c. Serum Albumin <2.5 gm/dl
2. End-Stage Liver Disease is present, and the patient has one or more of the following conditions:
- Ascites, refractory to treatment or patient declines or is non-compliant
- History of spontaneous bacterial peritonitis
- Hepatorenal syndrome (elevated creatinine with oliguria 1<400 ml/day)
- Hepatic encephalopathy, refractory to treatment or patient non-compliant
- History of recurrent variceal bleeding despite intensive therapy or patient declines therapy
Supporting evidence for hospice eligibility:
- Progressive malnutrition
- Muscle wasting with reduced strength
- Ongoing alcoholism (>80 gm ethanol/day)
- Hepatocellular carcinoma
- Hepatitis B surface antigen positive
- Hepatitis C refractory to interferon treatment
Lung Disease / COPD
The patient has severe chronic lung disease as documented by 1, 2, and/or 3:
1 a. Disabling dyspnea at rest
1 b. Poor response to bronchodilators
1 c. Decreased functional capacity (e.g., bed to chair existence, fatigue and cough), and
2. Progression of disease as evidenced by a recent history of increased visits to MD office, emergency room and/or hospitalizations for pulmonary infections and/or respiratory failure, and
3. Documentation within the past three (3) months of (a) or (b) or both:
- a. Hypoxemia at rest (p 02<55 mgHg by ABG) or oxygen saturation
- b. Hypercapnia evidenced by pC02>50mm Hg
Supporting evidence for hospice eligibility:
- Cor pulmonale and right heart failure secondary to pulmonary disease
- Unintentional progressive weight loss >10% over the preceding six (6) months
- Resting tachycardia >100 bpm
Multiple Sclerosis & Parkinson's Disease
The patient must meet at least one of the following criteria (1 or 2):
- Severely impaired breathing capacity with all of the following findings:
- Dyspnea at rest
- The requirement of supplemental oxygen at rest
- The patient declines artificial ventilation, or
- Rapid disease progression and either (a) or (b) below. Rapid disease progression as evidenced by all the following in the preceding twelve (12) months:
- Progression from independent ambulation to wheelchair or bed-bound status
- Progression from normal to barely intelligible or unintelligible speech
- Progression from normal to pureed diet
- Progression from independence in most or all
- Activities of Daily Living (ADL) to needing major assistance by caretaker in all ADL and
- a. Severe nutritional impairment demonstrated by all of the following in the preceding twelve (12) months:
- Oral intake of nutrients and fluids insufficient to sustain life
- Continuing weight loss
- Dehydration or hypovolemia
- Absence of artificial feeding, or
- b. Life threatening complications demonstrated by one or more of the following in the preceding twelve (12) months:
- Recurrent aspiration pneumonia (with or without tube feedings)
- Upper urinary tract infections (e.g., Pyelonephritis)
- Sepsis
- Recurrent fever after antibiotic therapy
- Stage 3 or 4 decubitus ulcer(s)
Renal Failure Chronic
The patient has 1 and either 2 or 3:
- The patient is not seeking dialysis or transplant, and
- Creatinine clearance* <1 Occ/min (15<cc/min for diabetics) or
- Serum creatinine >8.0mg/dI (>6.0mg/dI for diabetics) Supporting evidence for hospice eligibility:
- Uremia
- Oliguria (urine output is less than 400cc in 24 hours)
- Intractable hyperkalemia (greater than 7.0) not responsive to treatment
- Uremic pericarditis
- Hepatorenal syndrome
- Immunosuppression/AIDS
- Intractable fluid overload, not responsive to treatment
Appendix
New York Heart Association (NYHA) Functional Classification (Class & Description)
- Patients with cardiac disease, but without resulting limitation of physical activity. Ordinary physical activity does not cause undue fatigue, dyspnea, palpitations or anginal pain.
- Patients with cardiac disease resulting in slight limitation of physical activity. They are comfortable at rest Ordinary physical activity results in fatigue, dyspnea, palpitations or anginal pain.
- Patients with marked limitations of physical activity. They are comfortable at rest. Less than ordinary physical activity causes fatigue, palpitations, dyspnea or anginal pain.
- Patients with cardiac disease resulting in inability to carry on any physical activity without discomfort, Symptoms of heart failure or of the anginal syndrome may be present even at rest. If any physical activity is undertaken, discomfort is increased.
Strength Through Partnerships: Our Affiliations with Leading Healthcare Institutions and Hospice Organizations
At Allegiance Hospice we believe in the power of collaboration and partnership to provide the highest quality care to individuals facing end-of-life journeys. Through our affiliations with major hospitals, healthcare facilities, and hospice organizations, we strengthen our commitment to excellence, compassion, and support for patients and families. Here’s a glimpse into our valued partnerships:
Affiliations with Major Hospitals, Physicians & Facilities:
- Hospitals: Our partnership with HCA Houston Hospital & Kindred Hospital system allows for seamless transitions between hospital care and hospice services. We collaborate closely with the hospital’s medical team to ensure continuity of care and support for patients transitioning to hospice care.
- Long Term Care & Assisted Living Facilities: As an affiliated hospice provider with major Long Term Care & Assisted Living Facilities, we have access to advanced medical resources and expertise to meet the complex needs of our patients. This collaboration enables us to provide comprehensive care in coordination with the medical center’s services.
- Physicians & Specialist Practices: We work closely with major Primary Care Physician as well as Specialist Practices and to support patients in their palliative care journey, whether they are receiving palliative care during routine services or transitioning to hospice care. Our collaboration ensures a continuum of care focused on improving quality of life and function.
Partnerships with Hospice Organizations:
- Texas & New Mexico Hospice Organization (TNMHO): We are proud to be affiliated with the Texas & New Mexico Hospice Organization, advocating for quality hospice care at the state level and collaborating with other hospice providers to address legislative and regulatory issues affecting end-of-life care in our community.
Accreditation of Excellence
- Accreditation Commission For Health Care (ACHC): At Allegiance Hospice, we are accredited by Accreditation Commission for Health Care. Having an ACHC accreditation is a seal of excellence representing high quality of care delivered to our patients and families while ensuring high standards of regulatory compliance requirements by State & Federal level guidelines.
Why Our Affiliations Matter:
- Access to Resources: Our affiliations with major hospitals and healthcare facilities provide access to advanced medical resources, technology, and expertise to meet the complex needs of our patients.
- Continuity of Care: Collaboration with hospice organizations ensures seamless transitions between healthcare settings and hospice care, promoting continuity of care and support for patients and families throughout their journey.
- Commitment to Excellence: Affiliation with reputable hospice organizations demonstrates our commitment to upholding the highest standards of hospice care and continuously improving our services through education, training, and collaboration.
Join Us in Making a Difference:
At Allegiance Hospice, we are proud to collaborate with leading healthcare institutions and hospice organizations to provide compassionate, comprehensive care to individuals and families facing end-of-life journeys. Together, we are committed to making a difference in the lives of those we serve, offering comfort, dignity, and support during their time of need.